An excerpt from the 2024 Family Medicine Update Oct. 23 – 25.

Four Cardiology Subjects Primary Care Providers Need to Know
With advances in cardiology moving at a fast pace, it’s essential for primary care providers to stay informed. This article explores four areas of cardiology that impact primary care.
1. Cholesterol-Lowering Therapies: Moving Beyond Statins
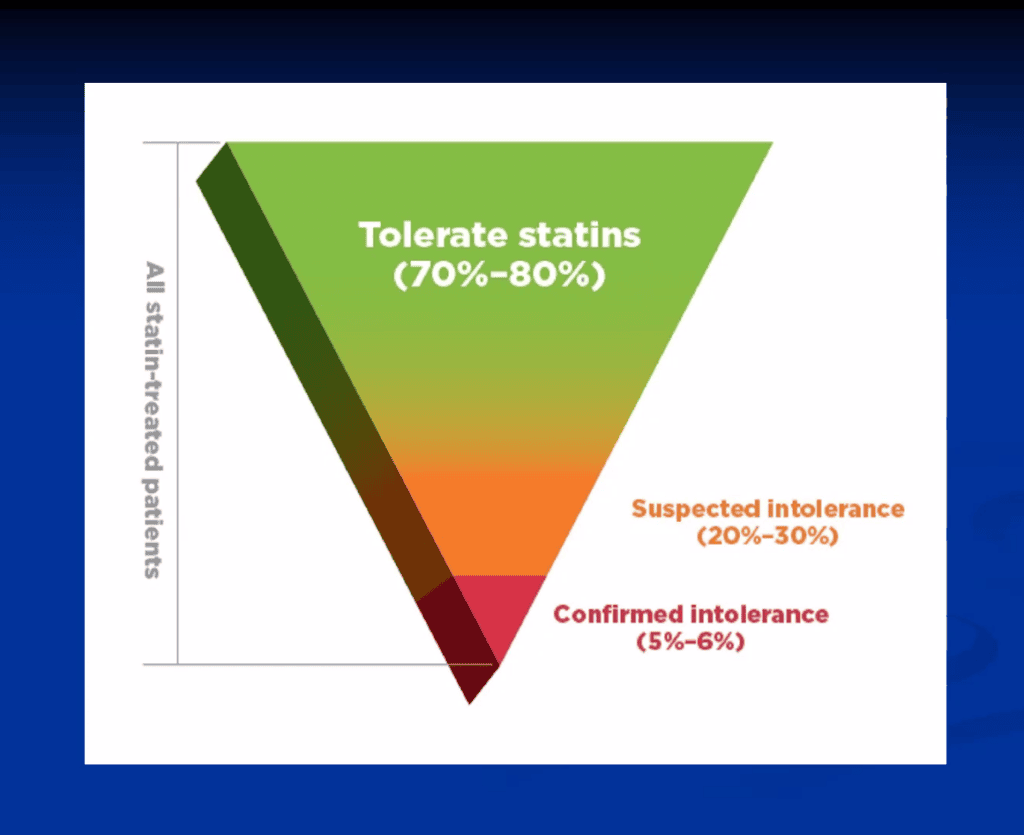
Statins have been a cornerstone of cholesterol management for decades, lowering LDL cholesterol and reducing cardiovascular events. However, about 5% to 6% of patients experience muscle pain or other side effects that make statins intolerable. These newer therapies offer promising alternatives:
- Ezetimibe: This medication reduces cholesterol absorption in the small intestine. When used alone, ezetimibe can lower LDL from 15% to 25%. It is especially beneficial for patients who are already on statins but haven’t achieved their target LDL levels. Studies show that combining ezetimibe with statins can improve cardiovascular outcomes by reducing the risk of heart attacks and other events.
- Bempedoic Acid: Approved by the FDA around 2019, bempedoic acid targets the same cholesterol synthesis pathway as statins but works earlier in the cycle, which may reduce muscle-related side effects. Bempedoic acid alone can lower LDL by 20% to 30%, and when combined with ezetimibe, it can be reduced by up to 50%. However, more outcome data are needed for wider adoption since larger trials won’t be available until 2026.
- PCSK9 Inhibitors: These injectable medications have become crucial for high-risk patients who can’t meet their LDL goals with just statins. PCSK9 inhibitors block a protein that limits LDL receptors, reducing LDL by about 50%. Although patients were at first resistant to an injectable form, they’re now more familiar with injectable medications such as GLP-1 agonists, which has improved acceptance. Access and cost have also improved.
- Inclisiran: This is another injectable option, lowering LDL by about 50% using mRNA technology to silence the production of PCSK9. The injection is twice a year, which suits patients who prefer infrequent dosing over daily pills. However, it is not widely prescribed because of limited cardiovascular outcomes data, which is expected in 2025.
2. Cardiac Electrophysiology and Atrial Fibrillation
Atrial fibrillation (AFib) is the most common arrhythmia, affecting about 5.6 million people in the United States. The American College of Cardiology, the American Heart Association and the Heart Rhythm Society have updated guidelines for AFib, emphasizing “pre-AFib” (early warning signs) and risk-factor modification to prevent AFib.
Risk Identification and Prevention
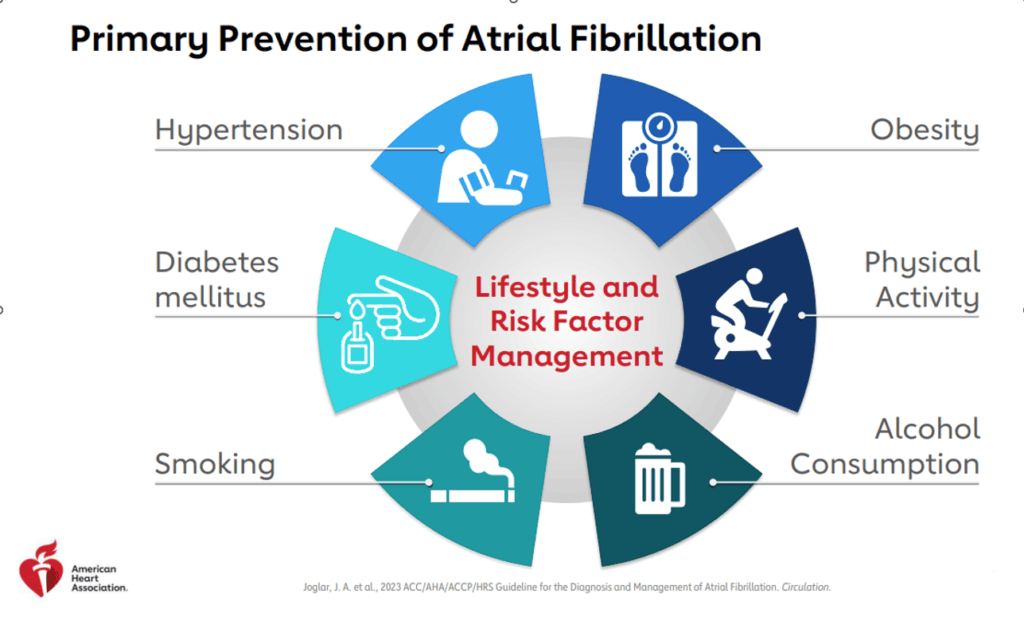
AFib is associated with several risks, including a higher chance of stroke, heart attack and cognitive decline. Understanding early markers of AFib—such as atrial ectopy (extra heartbeats) or short episodes of atrial tachycardia—can alert primary care providers to patients who may benefit from early intervention. Addressing modifiable risk factors such as obesity, high blood pressure and sleep apnea can potentially prevent or delay AFib.
Primary and Secondary Prevention
Managing AFib goes beyond heart rhythm control to reducing the patient’s stroke risk and minimizing AFib recurrence. Interventions include:
- Weight Loss: Weight loss significantly lowers AFib episodes and improves the success of procedures such as ablation.
- Exercise: Engaging in regular, moderate to vigorous exercise can help patients maintain sinus rhythm.
- Sleep Apnea Screening: Many AFib patients struggle with sleep apnea. Regular screening and potential CPAP treatment or other interventions can help. Though its benefits for sinus rhythm aren’t fully confirmed, treating sleep apnea can improve overall cardiovascular health.
Antithrombotic Therapy
AFib patients face a higher risk of stroke, particularly if they score high on the CHA₂DS₂-VASc scale. New guidelines recommend:
- Annual CHA₂DS₂-VASc Assessment: Regular updates to this score can help pinpoint patients who have moved from a lower- to higher-risk category.
- Direct Oral Anticoagulants (DOACs): Preferred over warfarin, DOACs reduce stroke risk with fewer side effects and monitoring requirements.
- Avoiding Aspirin: Studies have shown that aspirin monotherapy does not reduce stroke risk and can increase bleeding, making it an ineffective and potentially harmful option.
For patients at high stroke risk who cannot take anticoagulants, left atrial appendage occlusion devices (like WATCHMAN or Amplatzer Amulet) are now widely used. These devices help prevent stroke by closing off the area of the heart where blood clots most often form in AFib.
3. Congestive Heart Failure
Congestive heart failure (CHF) with preserved ejection fraction (HFpEF) is becoming more common, driven by factors such as aging, obesity and metabolic syndrome. Unlike heart failure with reduced ejection fraction (HFrEF), HFpEF is often related to conditions that affect the heart’s filling function rather than its pumping ability. This form of heart failure is challenging to diagnose and treat.
Diagnosis and Monitoring
Diagnosing HFpEF is complicated in that symptoms such as shortness of breath show up in many conditions, including lung disease and obesity. A helpful tool for diagnosing HFpEF is the H₂FPEF score, which considers factors such as high BMI, hypertension, age, symptoms such as atrial fibrillation and echocardiogram findings.
BNP and NT-proBNP levels, common markers in heart failure diagnosis, are less reliable for HFpEF, especially in patients with higher BMI.
Treatment Strategies
Treatment options for HFpEF have been limited, but new therapies have shown promise:
- SGLT2 Inhibitors: Originally developed for diabetes, these drugs are now first-line treatments for HFpEF, reducing the need for hospitalizations due to heart failure.
- Diuretics: For patients with fluid retention, diuretics can help relieve symptoms and reduce hospitalizations.
- Spironolactone and ARBs/ARNIs: These medications are considered secondary options and may benefit certain patients, though they do not reduce mortality rates.
Managing comorbidities is essential in HFpEF. Diabetes, obesity and physical inactivity can worsen outcomes.
4. Structural Cardiology: Minimally Invasive Interventions
Structural cardiology uses catheter-based procedures to repair or replace heart structures, allowing for less invasive treatments compared to traditional open-heart surgery. This field has expanded with new techniques for helping valve and rhythm issues in patients who are not ideal surgical candidates.
- Transcatheter Aortic Valve Replacement (TAVR): Once limited to high-risk patients, TAVR has become the preferred treatment for many patients with aortic valve disease. Since 2019, more TAVR procedures have been performed than traditional surgical valve replacements.
- Left Atrial Appendage Occlusion (LAAO): For AFib patients at high stroke risk who cannot take blood thinners, devices such as the WATCHMAN and Amplatzer Amulet close off the left atrial appendage where clots tend to form.
- Mitral Clip (TEER): In patients with severe mitral regurgitation who cannot tolerate surgery, transcatheter edge-to-edge repair (TEER) is minimally invasive and improves quality of life.
- Tricuspid Valve Replacement: A recent breakthrough is the percutaneous tricuspid valve replacement. This offers a new treatment option for patients with tricuspid regurgitation, a condition with limited effective treatments. Patients often see improvement in symptoms and fewer hospitalizations.