Evaluating Maternal and Neonatal Pharmacokinetics of CFTR Modulators

Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) modulators (elexacaftor/tezacaftor/ivacaftor) have revolutionized CF patient care, restoring normal function to people with CF (pwCF) who respond. Their use also quadrupled pregnancy rates in pwCF, a population where subfertility and maternal complications exist at a significantly higher rate. Pregnant women with CF have an increased risk for complications, including pulmonary decline. Consequently, they are advised to continue CFTR modulator therapy to prevent maternal deterioration, despite the lack of scientific evidence demonstrating their optimal dosing in pregnancy. As such, it is critical to define the pharmacokinetics of CFTR modulators in pregnancy and postpartum, including effects on the developing fetus, the infant, and breastmilk composition.
Unanswered Questions about CFTR Modulators Throughout All of Pregnancy
- How much CFTR modulator are babies exposed to in utero and during breastfeeding?
- How does pregnancy and postpartum affect CFTR modulator drug concentration?
Significance
Led by a team of Cystic Fibrosis and Maternal-Fetal Medicine investigators, we will enroll pregnant patients and their children to evaluate how pregnancy, postpartum, and childhood development influence CFTR modulator concentrations. We hope that The ELECTRA Pregnancy Study will generate rigorous CFTR Modulator pharmacokinetic data to inform optimal CFTR Modulator dosing and improve outcomes for pregnant patients with cystic fibrosis and their infants.
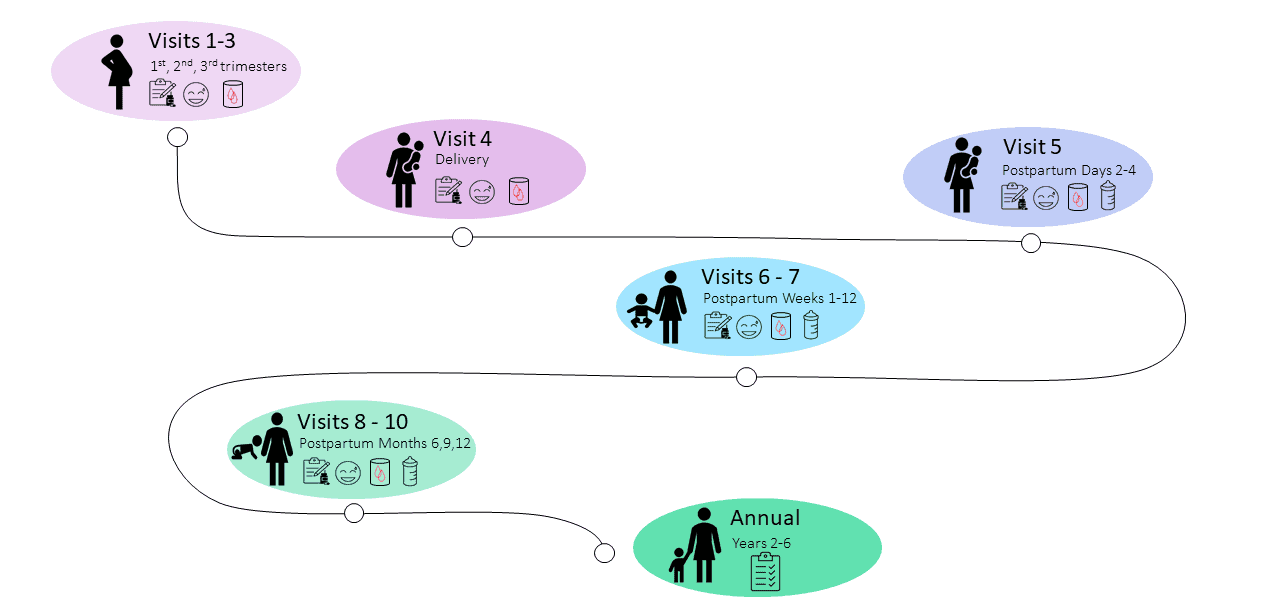
Study Procedures and Timeline
Recruitment Sites
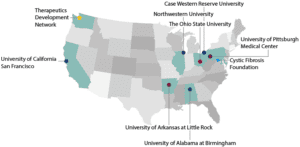
Recruitment Sites

University of Arkansas for Medical Sciences & Arkansas Children’s Hospital

University of Alabama at Birmingham

University of California San Francisco

The Ohio State University

Northwestern University

Case Western Reserve University
