Hirschsprung’s Disease
What is it?
A very common cause of low intestinal obstruction in the neonate (15-20%) (21), occurs with relatively higher frequency in boys and in infants with Down’s syndrome (21). These newborns often present with failure to pass meconium and abdominal distension (23). Although the causes are varied and quite different, ranging from imperforate anus, meconium plug syndrome, small left colon syndrome, colonic atresia/stenosis, and ileal atresia, Hirschsprung’s should always be in your mind when considering the many differentials. These babies are never born with normal ganglion cells in the myenteric neurons of the Meissner and Auerbach plexus (recall the bowel wall has many layers – 4 to be exact – starting from inside to outside, there is the mucosa, submucosa which contains the Meissner’s plexus, muscularis propria which contains muscles & the Auerbach’s myenteric plexus and lastly, the serosa) (24). This leads to a tight aganglionic segment with proximal dilation of the normal bowel (in this case, small and large bowel). It can result in functional obstruction due to spasm in the denervated colon (21). Ganglion cells arise from the neural crest and migrate through the intestines between the 7th – 12th weeks of gestation (23). This process is arrested in patients with Hirschsprung’s disease, and the neurons never completely reach the distal colon.
What do I need to know?
Patients often present with failure/delay in passing meconium, with signs of obstruction including abdominal distension, constipation, and vomiting. Enterocolitis and bowel perforation can complicate the straightforward presentation, often causing significant morbidity and mortality (21).
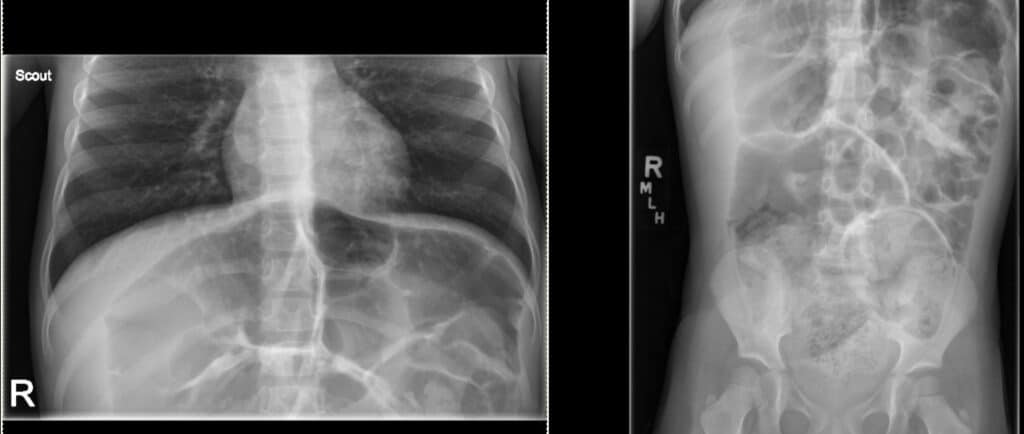
X-rays demonstrate radiological signs of bowel obstruction. The affected bowel segment is small while the proximal “normal” bowel is dilated.
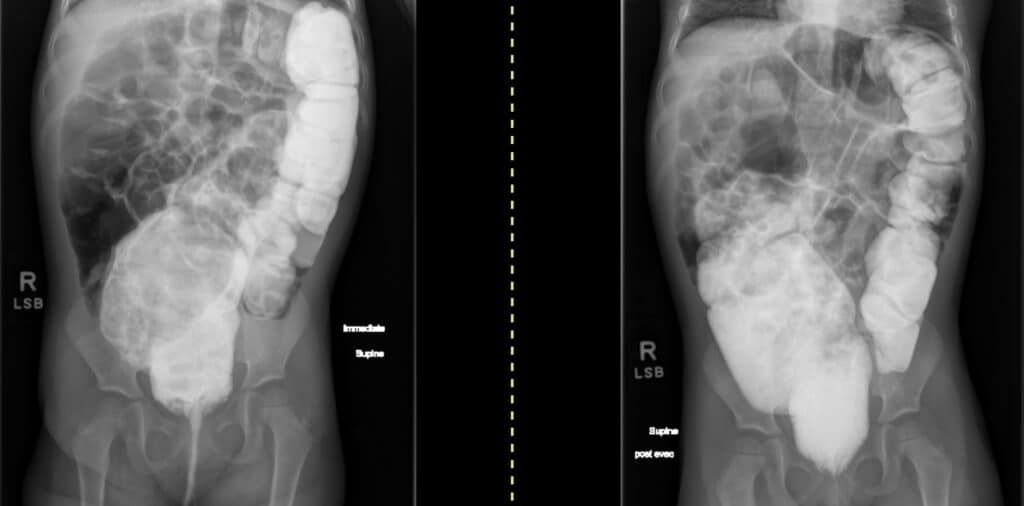
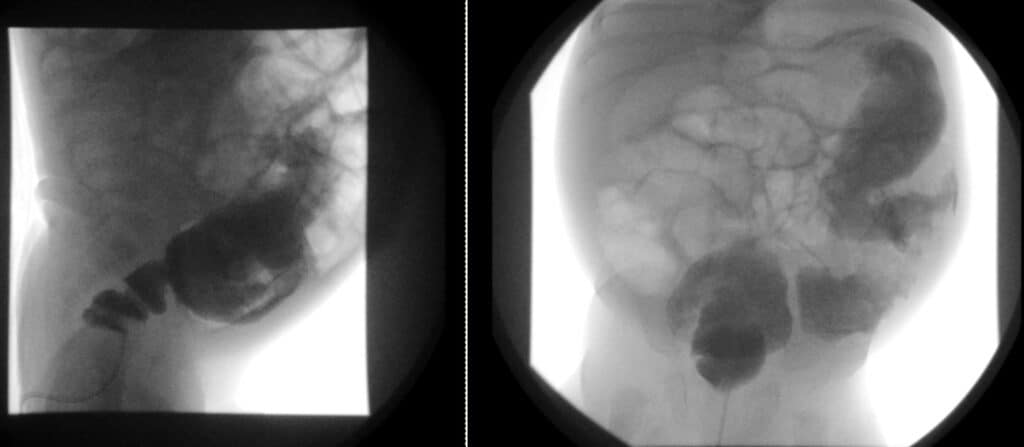
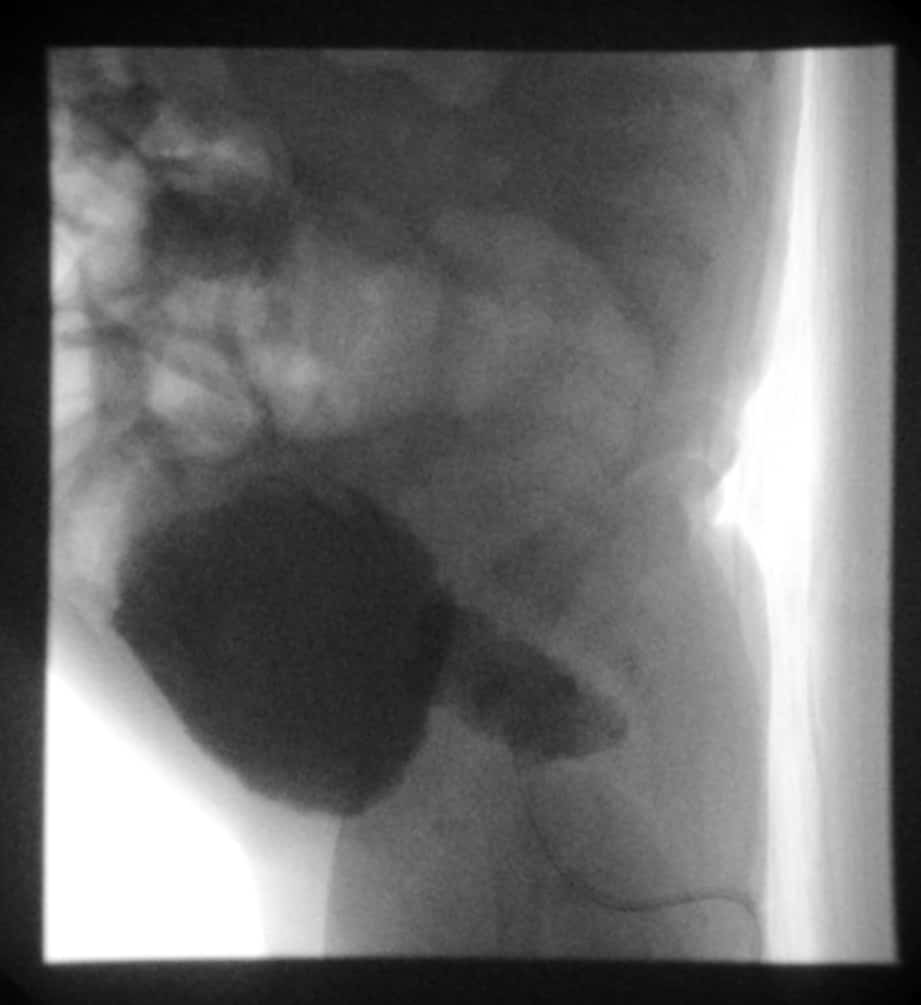
Diagnosis often relies on fluoroscopy guided contrast enema where the transition point is often clearly seen. Classic diagnostic signs to look for are the “saw-tooth” appearance of the aganglionic segment (impaired peristaltic waves) and reversal of the recto-sigmoid ratio (23). Normally, the rectum is often larger than the sigmoid colon (rectum is the largest part of the colon on the left) because the rectum functions as a reservoir, so the rectosigmoid ratio is >1. In babies with short segment Hirschsprung’s however, this ratio is flipped as the abnormal aganglionic rectum cannot distend and therefore, the sigmoid colon (“normal colon”) progressively distends proximally to accommodate the increasing stool burden.

Other things to consider when a newborn presents with dilated small bowel loops and a “low obstruction” are: meconium ileum, distal ileal atresia, colonic atresia, and small left colon syndrome.
Briefly, if you see a barium filled LONG MICROCOLON: think cystic fibrosis (CF) related meconium ileus (if contrast reaches the ileal loops) or distal ileal atresia (if contrast does NOT reach distal ileum – because there is no distal ileum, it did not form).
If you see a SHORT MICROCOLON, that is, barium filled narrow short distal colon and contrast never goes up, you’re probably looking at colonic atresia, likely secondary to an intrauterine vascular insult.
With a small left colon syndrome, you’d look for a caliber change in the colon: that is, a big distended ascending, transverse and proximal descending colon with a narrowed portion of colon involving the descending colonic segment (left colon). It is also called meconium plug syndrome, because it’s usually due to a meconium plug causing transient functional colonic obstruction in infants of diabetic mothers or mothers with eclampsia who received Magnesium Sulphate. Obviously, it’s self limited and resolves with contrast enema.
What do I need to do?
If you see an obstructive bowel gas pattern in a neonate who has not yet passed meconium with signs pointing to low intestinal obstruction, performing a barium enema is prudent. It is often the first exam to be requested/performed if there is concern for Hirschsprung’s disease (22). Of course, biopsy confirmation is always necessary, but you may be the one to push the clinical team in the right direction.
Selected References
21. Agrawal, R., Vadera, S. Hirschsprung disease. Reference article, Radiopaedia.org. (accessed on 13 Jul 2022) https://doi.org/10.53347/rID-1456O’Donovan A, Habra G, Somers S, Malone D, Rees A, Winthrop A. Diagnosis of Hirschsprung’s Disease. AJR Am J Roentgenol. 1996;167(2):517-20. doi:10.2214/ajr.167.2.8686640
22. O’Donovan A, Habra G, Somers S, Malone D, Rees A, Winthrop A. Diagnosis of Hirschsprung’s Disease. AJR Am J Roentgenol. 1996;167(2):517-20. doi:10.2214/ajr.167.2.8686640
23. Vivier, P., 2005. Hirschsprung’s disease in a neonate. [online] Eurorad – Brought to you by the ESR. Available at: <https://www.eurorad.org/case/3384> [Accessed 13 July 2022].
24. Rao JN, Wang JY. Regulation of Gastrointestinal Mucosal Growth. San Rafael (CA): Morgan & Claypool Life Sciences; 2010. Introduction.