Hypoxic-Ischemic Injury
What is it?
Neurological insult due to lack of adequate tissue perfusion. Accounting for up to 16-23% of death in pediatric intensive care units (1), brain death is usually clinically diagnosed with absent brainstem reflexes, coma and apnea in a patient with acute irreversible neurological insult.
How does it happen?
Global hypoxic injuries, which are devastating events causing death or significant neurological impairment, are often the underlying cause of pediatric brain death.
What do I need to know?
Although imaging appearance can be variable depending on the inciting traumatic event/cause, in most cases, specific patterns can be observed on imaging due to non-uniform affectation of the brain structures, as the gray matter is more susceptible to hypoxic insults (due to increased metabolic demand).
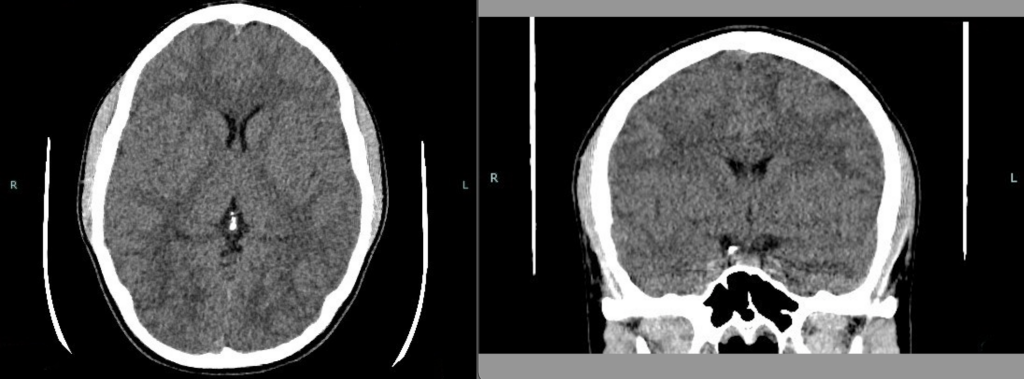
CT Findings:
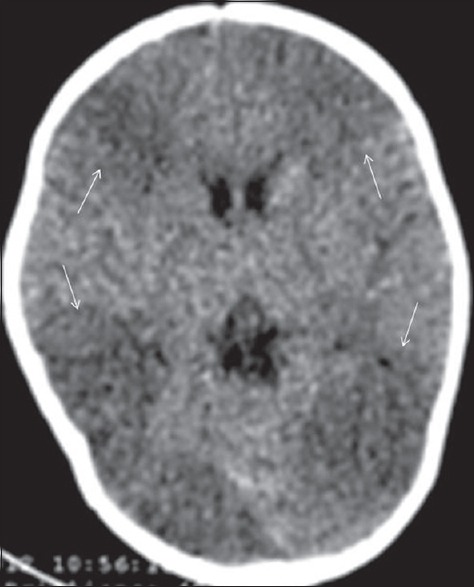
Although slightly less sensitive and specific than MRI, CT can be a useful tool to diagnose hypoxia in neonates. Normally, the deep gray matter structures including the thalamus, lentiform nucleus and head of the caudate nucleus are hyperdense when compared to the surrounding white matter and can be easily distinguished from the background low density white matter parenchyma due to preserved gray white matter differentiation. In hypoxia, the deep brain nuclei become hypodense due to cytotoxic edema caused by ischemia and acquire the same CT density as the surrounding white matter. As the ongoing ischemia worsens, and extensive diffuse cerebral edema develops, there is loss of sulcal spaces and generalized loss of gray white matter differentiation.
Source: Bano S, Chaudhary V, Garga UC. Neonatal Hypoxic-ischemic Encephalopathy: A Radiological Review. J Pediatr Neurosci. 2017;12(1):1-6. doi:10.4103/1817-1745.205646
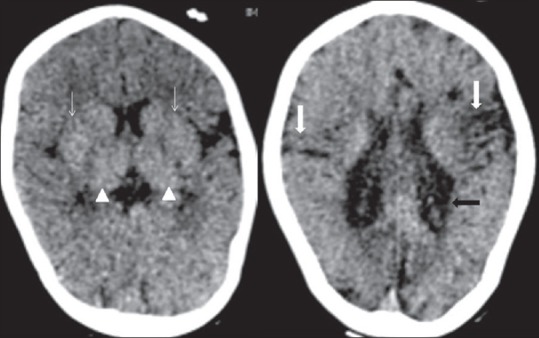
Noncontrast computed tomography head (axial) in a 3-year-old term male showing features of severe hypoxic-ischemic injury in the form of hyperdense basal ganglia (thin white arrow) and thalami (arrow head), loss of periventricular white matter, passive ventriculomegaly with irregular margin (thick black arrow) and atrophy of sensory motor cortex (thick white arrow).
Source: Bano S, Chaudhary V, Garga UC. Neonatal Hypoxic-ischemic Encephalopathy: A Radiological Review. J Pediatr Neurosci. 2017;12(1):1-6. doi:10.4103/1817-1745.205646
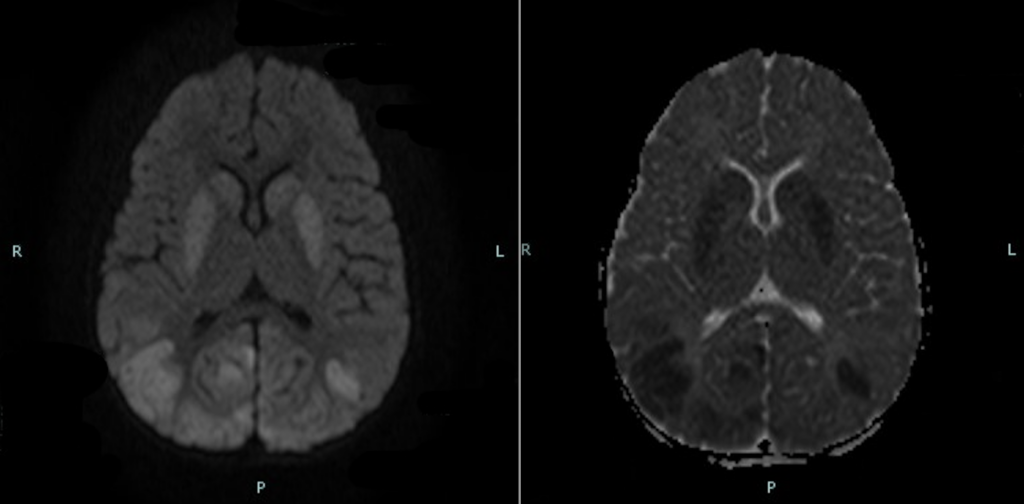
MRI Findings:
MR appearance of the neonatal brain is highly dependent on the myelination pattern. In a neonate who is at least 37 weeks of gestation, there is early myelination of the posterior limbs of the internal capsule which translates as increased signal intensity within the bilateral posterior limbs on T1 with corresponding decreased signal on T2. This finding is best appreciated within the first 24 hours (3). In contrast, the basal ganglia and deep gray matter nuclei are usually not T1 bright in a normal neonatal brain. Therefore, the four signs of neonatal hypoxia described in the literature include (2, 3):
- Absence of the posterior limb sign
- Abnormally increased signal intensity of the basal ganglia on T1 weighted images
- Abnormally increased signal within the thalami on T1
- Corresponding diffusion restriction within the deep gray nuclei
What do I need to do?
Call the care team to discuss the findings and document it on the preliminary report.
Selected References
1. Volakli, E. A., Mantzafleri, P., Kalamitsou, S., Violaki, A., Chochliourou, E., Svirkos, M., Kasimis, A., & Sdougka, M. (2017). Brain Death in Children. In N. Shaikh (Ed.), Intensive Care. IntechOpen. https://doi.org/10.5772/intechopen.68468
2. Huang, B. Y., & Castillo, M. (2008). Hypoxic-Ischemic Brain Injury: Imaging Findings from Birth to Adulthood. Radiographics, 28, 417–419. https://doi.org/10.1148/rg.282075066
3. Heinz, E. R., & Provenzale, J. M. (2009). Imaging Findings in Neonatal Hypoxia: A Practical Review. American Journal of Roentgenology, 192(1), 41–47. https://doi.org/10.2214/AJR.08.1321