Ingested Foreign Body
What is it?
Fairly common in the pediatric population, foreign body ingestion is usually seen in patients 6-36 months (2) as well as in older developmentally delayed children with incidence rates higher in boys and children <1 year of age (2, 18). Most frequently ingested items include coins, toys, jewelry and batteries with button batteries being the most common type (18).
What do I need to know?
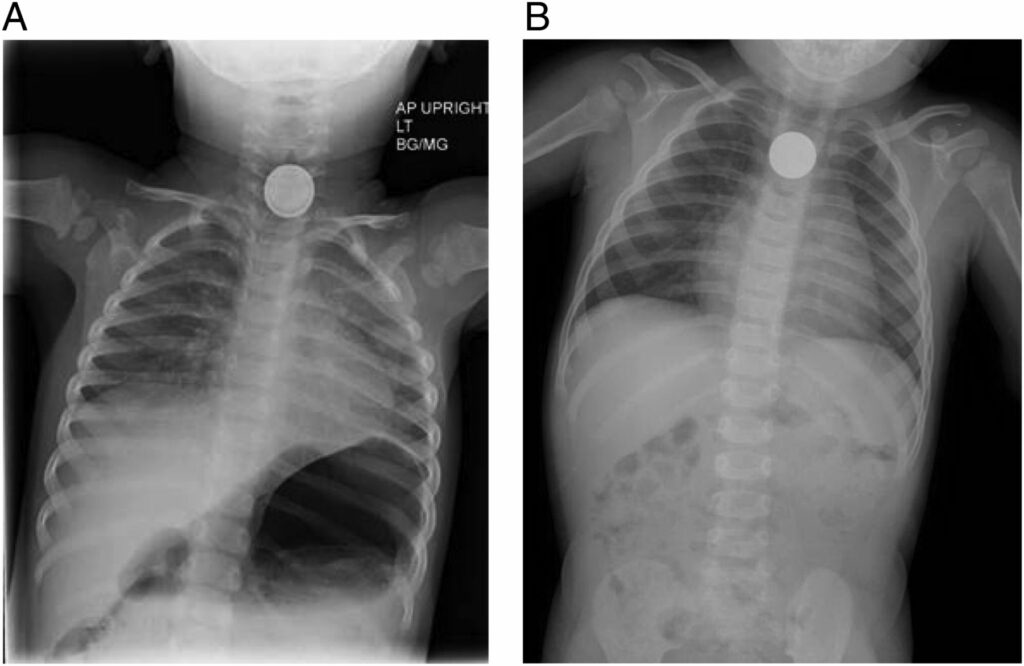
The first step is to differentiate between esophageal ingestion and tracheal aspiration as all airway foreign bodies are medical emergencies. Radiographically, flat foreign bodies orient in a specific plane indicating their location on AP and lateral chest x-rays. Tracheal foreign bodies will orient in the sagittal plane (e.g. –coins will look like flat radiopaque circles on lateral films) while esophageal foreign bodies will orient in the coronal plane (e.g. –coins will look like flat radiopaque circles on AP films). The size, shape, location and number of the foreign bodies should be specifically noted and dictated in the report.
There are 3 main areas in the esophagus where foreign bodies get trapped -thoracic inlet, aortic arch and gastroesophageal junction.
Decubitus views are very important to obtain in the case of non-radiopaque foreign bodies.
Although, the majority of ingestions are relatively harmless, there is significant morbidity and mortality caused by the ingestion of button batteries and magnets. Hydroxide radicals produced by the button battery lodged in the esophagus can cause caustic injury, necrosis, perforation, fistula and strictures in the esophagus. Look for the double edge sign to distinguish the button battery from a relatively harmless coin.
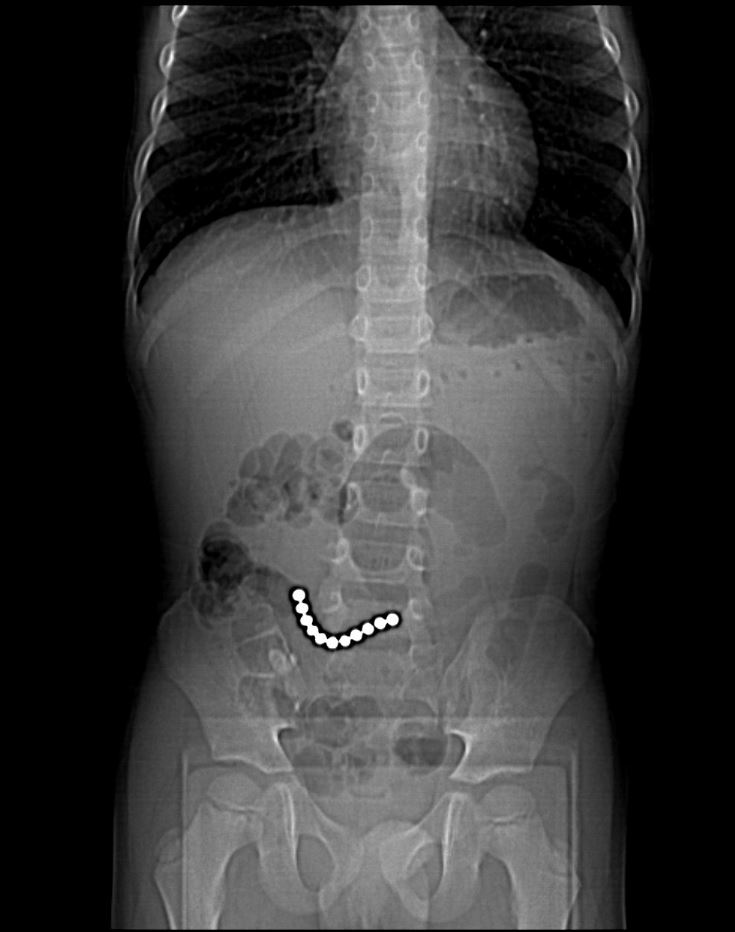
Similarly, ingestion of magnets should raise alarm because when more than one magnet is ingested, magnets will do what magnets know to do – attract each other -leading to a high risk of strong magnetic attraction between ingested magnets as well as pay attention to the magnets through the gastrointestinal walls leading to bowel entrapment which can cause obstruction, necrosis and perforation including entero-enteric fistulas, neatly summarized as “post gastric magnetopathy”.


What do I need to do?
If you see multiple magnets, note the location and number of ingested magnets as well as pay attention to the
- failure of movement of the magnets through the lumen on sequential radiographs
- gap between the magnets which can indicate entrapment and raise the possibility of ischemic injury to the intervening bowel (19).
Call the ED up and let them know to talk to surgery.
And to the same effect, if you suspect the child has ingested a button battery instead of an innocuous coin, make sure the ED knows.
Selected References
2. S., L. B., Amar, G., & Ellen, P. (2017). Imaging of Pediatric Gastrointestinal Emergencies. Journal of the American Osteopathic College of Radiology, 6(1), 5–14. https://www.jaocr.org/articles/imaging-of-pediatric-gastrointestinal-emergencies
18. Guelfguat, M., Kaplinskiy, V., Reddy, S. H., & DiPoce, J. (2014). Clinical guidelines for imaging and reporting ingested foreign bodies. In American Journal of Roentgenology (Vol. 203, Issue 1, pp. 37–53). American Roentgen Ray Society. https://doi.org/10.2214/AJR.13.12185
19. Wong, K., Van Tassel, D., Lee, J., Buchmann, R., Riemann, M., Egan, C., & Youssfi, M. (2020). Making the diagnosis of midgut volvulus: Limited abdominal ultrasound has changed our clinical practice. Journal of Pediatric Surgery. https://doi.org/10.1016/j.jpedsurg.2020.04.012