Nonaccidental Trauma
What is it?
Basically, child abuse. Radiologists can often be the first to suspect non accidental injuries as these cases are difficult to recognize clinically. Overt clinical signs and symptoms of physical abuse may be subtle, caretakers frequently provide an inconsistent and unreliable history and presentation can be mistaken for other common pediatric diagnosis.
What do I need to know?
Musculoskeletal injury may be the chief complaint in a child subjected to physical abuse and therefore, it is critical to have a high suspicion of index for non-accidental trauma. Skeletal surveys are usually performed in all cases of suspected abuse.
Pathognomonic MSK (and neuro) findings to be aware of on call include:
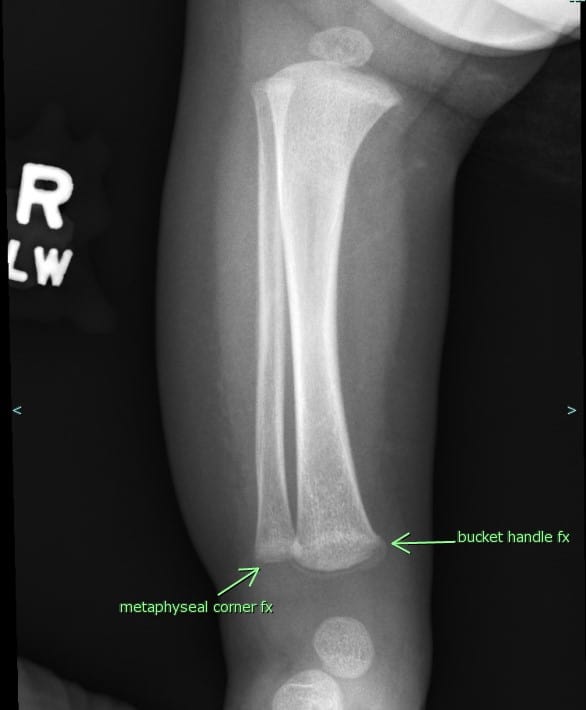
- Characteristic corner/bucket handle fractures (Metaphyseal corner fractures) Mechanism: twisting injury or torsion under traction with consequent separation of the corner piece of the metaphysis from the remainder of the bone – More a shaking type injury with limbs flailing.
- Fractures in hard to break places (scapula, spinous process, sternum)
- Rib fractures in multiple stages of healing (specifically, posterior rib)- Bilateral fractures

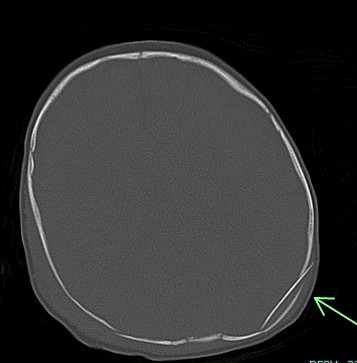
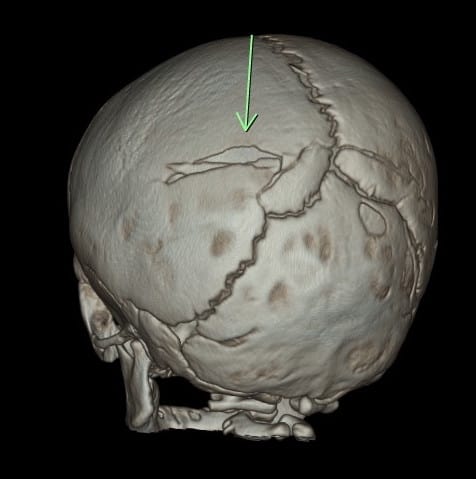
- Skull fractures (best to see them on 3D bone recons)
- Non parietal skull fractures
- Crossing suture lines
- Multiple bones
- Depressed skull fracture (signature fracture)

- Spiral humeral and femoral fractures


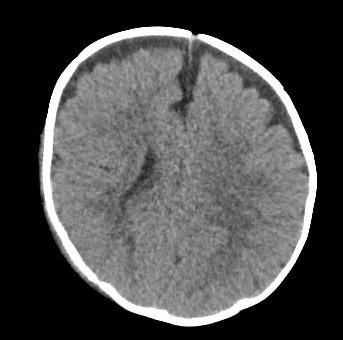
- Extra-axial hemorrhage (commonly subdural, may be epidural if associated with overlying skull fracture)

- Coup, contrecoup injury associated with parenchymal contusions, commonly in the temporal and frontal lobes adjacent to the petrous bone and posterior to the greater wings of sphenoid as well as superior to the orbital roof, planum sphenoidale and cribriform plate in the frontal lobe (use sagittal and coronal recons if available)
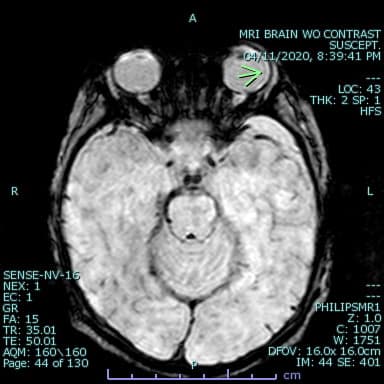
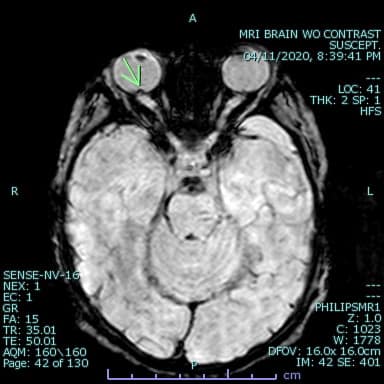
- Retinal hemorrhage (hard to see but can be seen in susceptibility images on MR as areas of signal loss within the vitreous)In case of suspected physical abuse in a child ≤24 months of age and/or a child presenting with one of the following: neurologic signs, apnea, complex skull fracture, other fractures or injuries highly suspicious for child abuse, suspected thoracic or abdominopelvic injuries, initial imaging evaluation includes a complete skeletal survey per the ACR appropriateness criteria revised in 2016.
What do I need to do?
If you see even one of the above listed findings, call the emergency department and discuss the findings with the ER physician and document it on the preliminary report.