Osteomyelitis
What is it?
Osteomyelitis refers to infection of the bone, bone marrow with or without extension into the surrounding soft tissues and classically presents with the cardinal signs of inflammation – fever, pain, swelling and loss of mobility. Commonly occurring in children < 5 years of age with nonspecific features (4), it can be challenging to diagnose. The most common site of infection is the metaphysis of the long bones, specifically the femur and the tibia(10).
How does it happen?
The metaphysis is the primary site of infection because of its unique vascular characteristics in the growing skeleton, namely abundant blood supply and capillary lakes or pools where bacteria can lodge and multiply (9, 10). For the first 18 months, there are transphysial vessels from the metaphysis to the epiphysis which traverse the physial plate, translating into a greater risk of spread of infection into the epiphysis and joint space which can result in septic arthritis. After 12 to 18 months, growth of dedicated epiphyseal nutrient vessel in the child and the concomitant disappearance of the transphysial vessels means that the physis can serve as a natural border to prevent the spread of infection from the metaphysis to the epiphysis and joint.
What do I need to know?
The diagnosis of osteomyelitis can portend significant changes to the patient’s management; therefore, it is critical to have answers to these three questions while reviewing imaging to make the most difference in patient care (9).
1. Infection – figure out if there is an infection
2. If yes, then where – localize the infection site
3. If yes, then how – estimate the burden of infection, see if there any drainable collections
Step 1
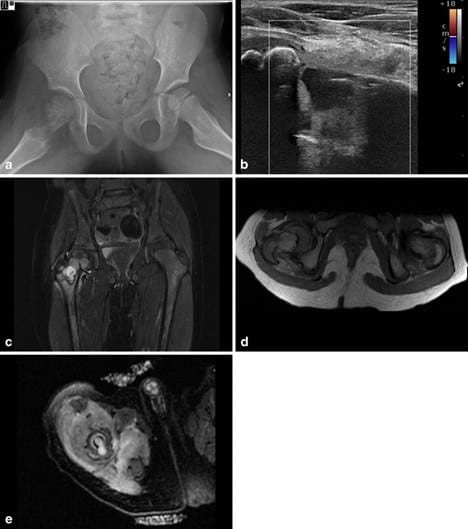
Radiographs are always obtained first but may not show changes in the early stages except for subtle soft tissue edema. Osteolysis and periosteal reaction are late findings that may take up to 7-10 days to appear, subacute changes include mixed lysis and sclerosis (4, 11). MRI with Gadolinium contrast is the modality of choice for prompt diagnosis of acute osteomyelitis. Any treatment delay can lead to a host of potential complications including septic arthritis, subperiosteal abscess, pyomyositis, deep vein thrombosis, chronic infection, and septicemia with impending death (9). Classically, osteomyelitis presents as decreased T1 and increased T2 signal (due to marrow edema) with enhancement of the affected area on contrast administration and significant surrounding soft tissue edema.

Step 2
The next step is to localize the site of infection to quantify disease burden and increase the diagnostic yield of tissue sampling (which is usually not necessary).
Step 3
The final step in the evaluation of osteomyelitis is to establish the presence or absence of drainable fluid collections which may require surgical drainage besides standard surgical debridement of the affected site. Note any intraosseous abscesses –which will appear as an area of high signal intensity in the bone on STIR and T2 weighted images and as a non enhanced center surrounded by rim of enhanced tissue on contrast enhanced images. Note any subperiosteal collections –which will appear as high signal intensity fluid collections trapped between the hypointense linear bony cortex and hypointense lifted off periosteum on T2 weighted and STIR images. On T1 weighted images, high signal intensity globules can sometimes be seen within the abscess, these correspond to fat globules which arise from the bone marrow fat and confirm the subperiosteal nature of the abscess (9).
Selected References
4. Bomer, J. and Holscher, H., 2020. The Radiology Assistant: Hip Pathology In Children. [online] Radiologyassistant.nl. Available at: <https://radiologyassistant.nl/pediatrics/hip/hip-pathology-in-children> [Accessed 8 August 2020].
9. Jaramillo, D., Dormans, J. P., Delgado, J., Laor, T., & St Geme, J. W. (2017). Hematogenous osteomyelitis in infants and Children: Imaging of a Changing Disease. In Radiology (Vol. 283, Issue 3, pp. 629–643). Radiological Society of North America Inc. https://doi.org/10.1148/radiol.2017151929
10. van Schuppen, J., van Doorn, M. M. A. C., & van Rijn, R. R. (2012). Childhood osteomyelitis: Imaging characteristics. In Insights into Imaging (Vol. 3, Issue 5, pp. 519–533). Springer. https://doi.org/10.1007/s13244-012-0186-8
11. Ciambotti, J., Lai, W., Cook, C., Altes, T., Casey, E., Pirttima, T., Pirttima, S., Mentore, K., HIgginbotham, J., Gupta, A., Mcllhenny, J. and Gay, S., 2020. Osteomyelitis. [online] Med Ed Virginia. Available at: < https://www.med-ed.virginia.edu/courses/rad/peds/ms_webpages/ms6bosteomyelitis.html> [Accessed 8 August 2020].